Instead of seeing your doctor or searching Google for answers to medical questions, how would you like a reference guide for nagging questions about your body?
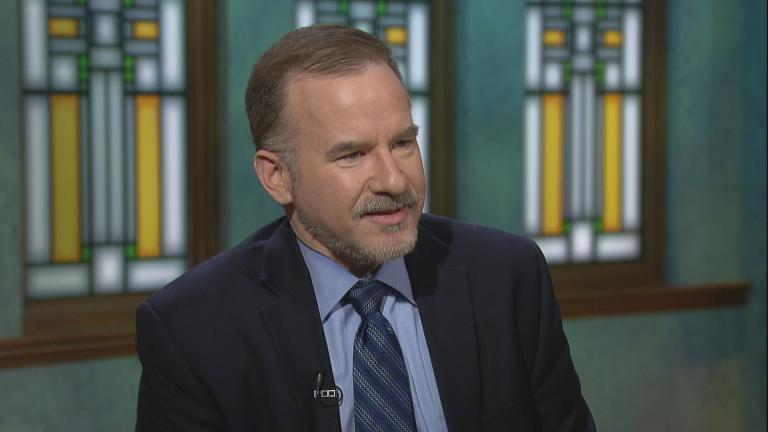
That’s the idea behind a new book from James Hamblin, a doctor and senior editor at The Atlantic. He hosts a series of web videos that answers a wide range of questions: How do I talk to strangers? Should I nap at work? Should I take a shower? Is wine healthy? Should I do yoga or Crossfit?
Hamblin’s new book, “If Our Bodies Could Talk: A Guide to Operating and Maintaining a Human Body,” collects, categorizes and answers some of the most persistent and interesting medical questions he’s received over the years.
Hamblin joins Chicago Tonight for a conversation.
Below, an excerpt from the book.
![]()
PROLOGUE
 My medical school roommate became an ophthal mologist and moved to Texas. He encouraged me to address here the most common question that people ask him in conversation when they learn his occupation:
My medical school roommate became an ophthal mologist and moved to Texas. He encouraged me to address here the most common question that people ask him in conversation when they learn his occupation:
If I lose a contact lens in my eye, can it get into my brain?
I laughed. He didn't. The question has lost its humor to him.
There are common, debilitating eye diseases that people could be asking him about-like macular degeneration, or night blindness. or glaucoma, which will affect 112 million people by 2040, leaving many without sight.
That last one resonates with me because I have it. The pressure inside my eyeball is higher than it should be. My eye won 't explode-though that image does absurdly haunt me. The decline in most glaucoma is, rather, insidious. I'm told I won't even notice as my eyes "fail"-a term that doctors use com monly, unthinkingly, until we're the ones whose parts are failing. It's more accurately the case that the pressure inside my eyes will gradually damage the dense focus of nerves in the retina at the back of my eye. I stand to slowly lose vision at the peripher ies of my field of view, and then entirely.
This won't happen for years.
Which is all to say that we have our reasons for concerns about our eyes and other parts. Every one is valid. Sometimes it helps to put them in the context of other people's problems-of how bad things could be. But sometimes it doesn't. So, to the question at hand: The space under our eyelids does not con nect to our brains. It's a cul-de-sac that ends about halfway over our eyes. Our brains are safe from contact lenses.
This anatomy is some thing you might have seen if you were among the forty million people who experienced the most popular traveling museum exhibition of all time: Body Worlds. Though you may have missed the cross sections of human heads if you were too distracted by the corpses that were posed having sex. That element of the exhibition shocked many attendees, as did rumors about dubi ous procurement of the bodies. Maybe most shocked was the art world, though, by the very fact of the enormous and endur ing popularity of an exhibit that might have been alternatively titled Actual Corpses.
Of all the art bestowed to us throughout history,why should what is essentially a glorified biology lab be so successful and adored? Especially as most of us are otherwise so averse to dis cussing so much of what our bodies do, and considering death, in any realistic way?
Body Worlds is the brainchild of the German anatomist Gun ther von Hagens, who invented the "plastination" process that allows bodies to be preserved without decomposing. While most exhibits come and go, Body Worlds has now been appear ing around the world for more than two uninterrupted decades. It even stays open on Friday nights to accommodate couples who want to make a date of it.
The marketing professor Kent Drummond at the University of Wyoming surmises that Body Worlds speaks to people because it manages to juxtapose our distaste for the abject with our desire to live forever. The displays draw on the sublimity of our mortality without leaving us feeling consumed by it. Drummond came to this understanding by studying not only the corpses but also living people as they move through the exhibition. He writes in a field note,"In one oft-repeated pattern of interaction, a man points to a body part in a casement, then explains to a woman how that part functions. He does so by showing her where it is on his body."
This masculine exhibitionism may be more sobering than the corpses themselves. It's also in keeping with the grand vision of Von Hagens, who identifies as a "medical socialist." He believes that health information should be a social good: the constella tion of factors that go into picking up a cigarette should include an abiding familiarity with a black, necrotic, emphysematous lung, which should not be exiled to textbooks and morgues. Inside Body Worlds, we can clearly see and contemplate our organs and their mortality, if only for one date night. Placards scattered throughout the exhibition urge self-reflection, such as Kahlil Gibran's "Your body is the harp of your soul."
I don't think that means anything, but Von Hagens's philos ophy does. Democratizing health information has become the norm well outside the walls of his exhibit. A past wor ld in which doctors were the keepers of all medical knowledge-whose job was primarily dispensing directives- is gone. Most of us are rather awash in information now-so much so that it can be dif ficult to know what to make of it.
Googling bodily concerns isn't always helpful. Anonymous people in forums can be found debating all things-including the great dilemma of the contact lens . (Can it get far into my eye to my brain and cause damage? What if it goes down my spine and into my shoe? Is it still safe to wear again?) And even when you find a reliable-looking source of health information, there is almost always a ready conspiracy theorist who writes with passion and anecdotal logic to warn everyone not to trust that source. Usually it's a guy on Reddit named Gene. Gene person ally lost five hundred contacts in his brain, and he had to have them surgically removed. He has the mass of desiccated contact lenses sitting in a jar on his desk.
While contact lenses can't get into our brains, they can in rare cases get stuck in the cul-de-sac above or below the eye ball. Like most anything that gets stuck in our bodies, this can be a source of infection. The pus around the contact lens can drain into a person's sinuses and spread into their pharynx. This has happened to me. I thought my contact had just fallen out, but no. Six days later, it came out. In the interim, I got pretty sick.
So, do seek medical attention if you have a trapped contact that is refusing to come out. (I hope everyone read this who le answer and not just the beginning.)
At Stanford University, the gaunt, bespectacled professor Rob ert Proctor teaches a course called "History of Ignorance." If he believed ignorance were simply the absence of knowledge, cured by imparting facts, his course would be dull. Instead, he argues that ignorance is the product of active cultivation. It spreads through marketing and through rumor, and it spreads much more easily than wisdom.
Contrasting his idea with the study of knowledge, epistemol ogy, Proctor has named the study of ignorance agnotology. The word is still not in the Oxford English Dictionary, though it is relevant to the dictionary's most recent Word of the Year, .
In 1977, a wide-eyed Proctor left home in Indiana to pursue a graduate degree in the history of science at Harvard. There he found himself "disturbed and puzzled" at the apathy that his professors had for "what ordinary people think ." He saw it partly as elitism; the rest was a darker sense of futility. "At the time, half of the country thought Earth was six thousand years old," he recalls. That's off by about 4.6 billion years. But more puzzling to Proctor than the discrepancy itse lf was the apathy toward it on the part of his colleagues in academia. So he decided that some one should study "what people don't know and why."
The classic example of purposeful ignorance is that created by the tobacco industry. Ever since tobacco was clearly proven to cause lung cancer in the 1960s, the industry has attempted to cultivate doubt in science itself. It cannot refute the facts of cigarettes, so it turned the public opinion against knowledge. Can anything really be known?
The strategy was brilliant. Proctor calls it "alternative causa tion," or simply, "experts disagree." Tobacco companies didn't have to disprove the fact that smoking causes cancer; all they had to do was imply that there are "experts" on "both sides" of a "debate" on the subject. And then righteously say that every one is entitled to their belief. The tactic was so effective that it bought the industry decades to profit while reasonable people were uncertain if cigarettes caused cancer.
As Proctor put it, "The industry knew that a third of all can cers were caused by cigarettes, so they made these campaigns that would say experts are always blaming someth ng-brussels sprouts, sex, pollution. Next week it'll be something else."
Once you start looking for this tactic, it's hard to miss. It's nowhere more common than in the messages about our bod ies. Proctor rattles off examples: vaccine agnotology, clitoral agnotology, food agnotology, milk agnotology. He likes to say we live in "the Golden Age of Ignorance." Because of the way information flows, "powerful agencies are able to create igno rance and spread lies through more vehicles than there have ever been in history."
Proctor is not alone in this thought: There's undeniably more scientific misinformation and marketing-based "facts" about our bodies coming at each of us daily than in entire lifetimes of generations past. And as we increasingly read only the articles that appear in our inboxes and curated social media feeds, "it's easier and easier," Proctor says, "to silo yourself into a tunnel of ignorance."
To allow ourselves to be challenged-to welcome it, and to seek it out-is to guard against the purposeful cultivation of igno rance. To be a doctor today is ever closer to its Latin root,docere ("to teach"), which I take to mean sharing habits of thought. The challenges for doctors and patients alike are in contextualizing, separating marketing from science, finding the lines between known and unknown, and discerning the motives of the people who attempt to define and redefine health and normalcy. If we all equip ourselves accordingly,we might reckon with the onslaught of bodily messages and maintain a solid understanding of our selves that allows us to relate productively to one another and move cogently, even happily, through the world.
So this book is a practical approach to understanding our bodies, predicated on the idea that memorizing facts is less important than developing insight. This is also a corrective to the approach that drove me away from practicing medicine. In premed courses, throughout medical school, and in the three years that I spent in residency, I memorized roughly infinity facts. During that time, it wasn't uncommon for people teach ing me to admit that Ijust needed to memorize these things to pass a test, that no doctors in the real world actually remember all this stuff-all the structures of amino acids, and the names of the small arteries that supply the elbow, and every possible minor side effect of every known medication. These are things that can be easily looked up at any moment. But still, on the exams that propel a person to success in the field, minutiae are currency.
After years of memorization, the overall effect was one of jumping through hoops w ith the explicit purpose of getting to the next hoop. My mentors advised me that if I didn't love the process by that point, I probably wasn't going to love the end result. So in 2012 I went on leave from the radiology residency at UCLA. I got the opportunity to take a job as editor of the health section of The Atlantic's digital magazine-a publication I had always read and loved. I was happier and more engaged, learn ing in a way that made sense to me.
So I resigned from UCLA. I justified leaving a very stable, lucrative career for a very unstable industry by the fact that there are not enough science journal ists or doctors working in public health. I wanted to have an impact on the roots of prob lems more than the symptoms,to question the textbooks rather than memorize them, and, ideally, to make people laugh. Jour nalism allows me to have some hand in public scientific literacy, and that might be, I mean to suggest with this book, the most valuable tool in pursuing health and happiness.
I've yet to regret my decision for any extended period of time.
The book began as a collection of straightforward answers to common questions about bodies, because, professionally and personally, I get a lot of those. It grew to interrogate those questions-why we care, or don't, about how our bodies work, and how our understandings of our bodies shape how we come to believe what's to be done about ourselves. At the root of the most virulent diseases and violent mistreatment of one another is ignorance, and much of that begins with fundamental mis understandings of our differences- understandings of ourselves and others that begin with our bodies. The questions in this book often began with little more than minor bodily curiosities, which, looked at more closely, are not at all minor.
Many of the answers are, rather, stories about why we don't have concrete answers. Sometimes the most interesting thing is knowing why we don't know, and the point is in the consider ing, and being comfortable in not knowing. Health is a balance between acceptance and control.
What is normal?
Too many daily decisions about what to put into our bodies how to put what in where, and what to do with that body once it's full of things-come down to vague ideas of what is good or bad, healthy or unhealthy, natural or unnatural, self or other. In a world of inordinate complexity, we instinctively attempt to put things into these binary categories.
University of Pennsylvania psychologist Paul Rozin believes that we do this to help maintain a sense of order. He calls this instinct "the monotonic mind." Even though we know better, we tend to resist the idea that most things are beneficial in some contexts or amounts, and harmful in others. It's easier to regard things as simply bad or good, to be adored or avoided.
In that tendency to seek order and control,an abiding theme among bodily questions and concerns is the concept of normal. The word tends to mean different things to scient ists, who use it in every other sentence, with statistical deviation in mind, and nonscientists, who are more likely to hear in it judgment.
Is it normal that I can bend my finger all the way back until it touches my wrist? Statistically, no. That doesn't mean it has implications for your health.
Maybe more consequential than its normalcy is the simple fact that if you're able to do that, you probably also know that people don't like watching it. The Canadian psychologist Mark Schaller argues that we're wired to be averse to looking at things like people flipping their eyelids inside out-to say noth ing of injuries like bones broken or blood outside of vessels because of a concept called the "behavioral immune system." We're repelled because on some level we sense a threat to our health.
Clearly, if our reactions to eyelid flipping or finger flexibility are an indication, our behavioral immune system is far from per fect at acting on only credible threats. Schaller has implicated this faulty self-preservation instinct in all sorts of behaviors, which lead us to isolate ourselves into cliques and communities based on the appearances and funct ions of our bodies.
At a grander scale, then, the system he proposes can be seen to be involved in many of the world's fundamental divides (rac ism, ageism, xenophobia). It stems from our understanding of ourselves-which, again, begins with our bodies. Understanding oneself as abnormal can register anywhere between liberating and suffocating.
Or the idea of "normal" can be rejected altogether. A central tenet of the Deaf community, for one, is that deafness should not be considered a disease to be treated or cured. The community does not consider people to be hearing "impaired" and rejects any reference to hearing "loss." The same is true for some other communities long marginalized by some bodily process.
Still, even as normalcy is a loaded concept, it's sometimes a necessary lens through which to understand disease and, ulti mately, to reduce suffering. Identifying outliers is central to the study and improvement of health. Science can't skirt the con cept of normalcy, and neither can this book. But I do my best here to separate statistically common ways of being from judg ments of value, of right or wrong, of implying that there is some ideal way to operate, look, feel, or be.
What is health?
At the founding of the World Health Organization in 1948, the group's constitution defined health in a way at once obvious and radical: "A state of complete physical, mental, and social well being, and not merely the absence of disease or infirmity."
With that, the World Health Organization hoped to inspire a new purview for the medical profession.
It failed. In much of the world, "health care" systems still today focus exclusively on the absence of disease or infirmity.
More specifically, they focus on treating disease after it already exists. In the last few years, though,an upheaval has begun.
The spring of 2015 saw the swearing-in ceremony of Vivek Murthy, who was quickly among the most controversial U.S. sur geons general. Conservat ive politicians attempted to block his appointment because of a tweet three years prior. Murthy had written, "Tired of politicians playing politics [with] guns, putting lives at risk [because] they're scared of NRA. Guns are a health care issue."
It wasn't even an especially revelatory tweet. Homicide and suicide are perennially among the leading causes of death in the country, a fact that has recently led the American Medi cal Association and other physician bodies to recommend that doctors ask all patients as a standard screening question-just as they should ask if patients wear seat belts and have fire extinguishers-if they keep guns in their homes. But it was the sort of tweet that can keep a person out of political office, in a country where the National Rifle Association and its elected officials have forbidden the Centers for Disease Control and Pre vention from even studying gun violence.
After a harrowing welcome to politics, Murthy ultimately made it through confirmation. When he took the podium to be sworn in, he spent little time talking about the traditionally paradigmatic doctorly pursuits-treating pancreatitis, perform ing colectomies or cardiac ablations. Actually, no time on those things. He underscored instead how preventable illness influ ences and is influenced by education, employment, the environ ment, and the economy. He called for the building of "the great American community" that will approach health as a unified endeavor.
His words build on a growing movement in the medical pro fession. While the United States spends the most money per person on health care of any country, it ranks forty-third in life expectancy. And more important than longevity, the United States is near the bottom of the ranking list among wealthy countries in personal health status. In a pivotal 2007 paper in the New England Journal of Medicine, physician Steven Schroeder argued that medical care accounts for only about 10 percent of what determines a person's likelihood of dying young. Genetic factors might account for another 30 percent or so. The remain ing 60 percent came down to social and environmental circum stances and behaviors. These are necessarily rough estimates, but they serve to push back against the way of thinking that leads us to think about hospitals, pills, and procedures when we think about improving health. Schroeder argues in the journal, "Even if the entire U.S. population had access to excellent medi cal care-which it does not-only a small fraction of [premature] deaths could be prevented."
This is not to say that modern health care cannot accomplish amazing things in treating diseases, some of which I'll get into in these pages, but that we rely too heavily on a mind-set where our system fixes problems, and not heavily enough on creating systems where these problems do not arise.
Over the decades, physicians have tended ever more toward specialties (and subspecialties, and sub-subspecialties) that treat discrete organ systems-dermatologi c oncology, pediat ric autoimmune gastroenterology, neuro-oncology, and so on whic h has been critical to managing the wea lth of information as science advances. But it has also left behind comprehensive approaches to the conditions that sicken and kill most people, first among them being the disease that we vaguely call "meta bolic syndrome." This manifests as a combination of obesity, dia betes, and cardiac death. This is primarily a disease of society, a disease of life.
As patients, the concept can be liberating: Our control over our health is great. And, more interesting, our ability to improve the health of others is great.
A typical textbook of anatomy and physiology is still today broken down by organ systems, based on physical structures. But when it comes to health and disease, organ systems are rarely affected in isolation. Distinctions like "heart health" and "brain health"-the sort still made on everything from cereal boxes to infomercials to ranking of academic medical centers are outdated. So Idivided this book not by traditional organ sys tems, but by categories of use. Most of the entries can be read in isolation but make the most sense in the context of the others, as read sequentially.
Overall, the book is predicated on something closer to the 1948 definition of health. It is drawn from my experience as a physician and journal ist, and the people I've had the opportunity to meet throughout the course of my career so far,and whatever wisdom I gained from knowing them.
Reprinted with permission from “If Our Bodies Could Talk: A Guide to Operating and Maintaining a Human Body.”
Related stories:
 Neil Steinberg Shares Advice, Sobering Quotes on Addiction in New Book
Neil Steinberg Shares Advice, Sobering Quotes on Addiction in New Book
Dec. 21: The Chicago Sun-Times columnist muses on weathering the holidays without alcohol and his anthology on addiction, “Out of the Wreck I Rise: A Literary Companion to Recovery.”
 Author Mary Roach on ‘The Curious Science of Humans at War’
Author Mary Roach on ‘The Curious Science of Humans at War’
Oct. 31: Serving in the military can be dangerous, frightening and unpleasant – sometimes in ways you might not expect. How the military tackles loud sounds, bad smells and upset stomachs.
 Sniff it Out: New Book Follows Dogs ‘Into a World of Smell’
Sniff it Out: New Book Follows Dogs ‘Into a World of Smell’
Oct. 20: From service dogs to household companions, a new book looks inside the complex world of a dog’s nose.

")
")


{kind=link}